If you are looking for an alternative to the PDSA model for quality assurance/quality improvement (QA/QI) in healthcare, you’ve come to the right place! The good news is that I have created an alternative to the Plan-Do-Study-Act (PDSA) model that predominates the QA/QI space in healthcare. Unlike the PDSA model, my model is evidence-based, and works for all functions of QA/QI departments in healthcare!
But I am forced to be honest. The bad news is that my alternative is just as hard – maybe even harder – than the PDSA. In this post, I’ll apply both my model and the PDSA model to an example so you can see how it works.

Alternative to the PDSA Model: Application to AHRQ Health Literacy Example
As we all know, healthcare is a team sport. In my last post in this series, I linked you to a web page by the United States Agency for Healthcare Research Quality (AHRQ) that described using the PDSA to quickly test a health literacy tool for implementation in a clinic. But if you are trying to improve health literacy among patients in your entire healthcare system, AHRQ’s description suggests that the PDSA cycle might be able to be used focally in the process, but would not account for all functions of QA/QI.
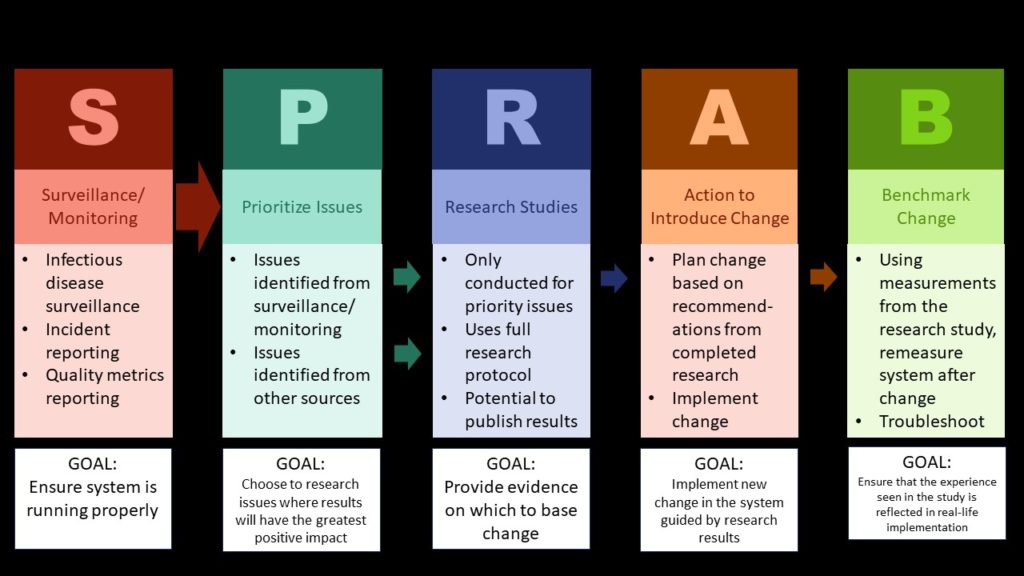
Unlike the PDSA, my model delineates the five functions of a QA/QI department in healthcare: Surveillance, prioritizing issues, doing research studies, action to introduce change, and benchmarking change. Let’s imagine that we run a QA/QI department, and want to improve the health literacy of the patients using our healthcare system. Let’s do a tabletop exercise to figure out how trying to improve health literacy in our healthcare system might relate to 1) the five functions of a QA/QI department from my model and 2) the stages of the PDSA model.
- Baseline Measurements: First, we would have to benchmark (fifth function) the existing level of health literacy. Literally, we’d have to pick a health literacy tool and measure a bunch of patients of the healthcare system. The reason this is an act independent of the PDSA is that we need this information before we even make a “plan”. What if health literacy is already at 100%? Then we wouldn’t need to do the PDSA. Or what if just a subset of the population has low health literacy? How would we know without starting with basic epidemiology? That doesn’t apparently fall in the PDSA. This also reflects another function of a QA/QI department, which is to prioritize issues (second function).
- Prioritizing: If our research shows health literacy is high enough, we might stop there. But if we felt we needed to improve it and we wanted to do an intervention, we’d have to do some more research (third function) first. Perhaps the “plan” in the PDSA could be a research plan for this intervention. But what if research shows our proposed intervention didn’t work? We’d have to continue to do research until we got a viable solution that we could roll out to the healthcare system. This might mean doing a series of different studies to figure out everything we’d need to know. Perhaps this was what the PDSA was getting at – but even so, each study needs to use a study design that is appropriate to the research aim, so the PDSA does not provide any guidance from that standpoint.
- Leadership Functions: Third, if we actually did all the research we needed to answer our questions about health literacy in our patients, the next step is that we’d have to make some big decisions, which are basically functions of QA/QI leadership. If we decide we are going to do action to introduce change (fourth function), we’d have to also come up with a way of benchmarking change (fifth function) to make sure we were getting our ROI from making the change. If the problem was especially important, like falls, then we might prioritize it (second function) and track it with surveillance (first function). Or else, we might not see that it meets the priority of surveillance, so we just make a plan to benchmark the change. Some of these activities – actions, measuring change, etc. – might be reflected somewhere in the PDSA, but the PDSA could not really guide this part.
My Way vs. the PDSA Model for QA/QI in Healthcare
The main difference between my alterative to the PDSA model and the original model is that my way is actually guaranteed to work if you do it right. It’s using classic epidemiology and biostatistics to arrive at root causes of quality issues in healthcare, rather than an old engineering management approach, which is what the PDSA is based on. Since epidemiology was invented to figure out root causes of co-morbidities and mortality, why not use this same set of tools to figure out root causes of problems in the healthcare system?
But it is hard to learn epidemiology and biostatistics, so it’s not like my alternative is easy. The main difference between my alternative and the PDSA is that my alternative always eventually works if you do it right, and it is appropriate for every setting. As I described before, it is unclear that the PDSA model works for most applications in healthcare, and it does not seem to account for all functions of a QA/QI department in healthcare. My approach works in all settings inside and outside healthcare, and not only accounts for but actually honors all functions of the QA/QI department.
Updated July 19, 2021 (added slider menu). Updated links and revised banners on June 21, 2024.
Read all the posts in the series!
Quality Improvement in Healthcare: What is the PDSA Model, and How Well Does it Work for QA/QI? Part 1 of 5
Wondering what the Plan-Do-Study-Act (PDSA) Model is, and if you should adopt it for quality [...]
Jun
The Stages of the PDSA Model: What do they Really Mean? Part 2 of 5
What are the stages of the PDSA model, and how do they relate to the [...]
Jun

Does the PDSA Model Work? Part 3 of 5
The Plan-Do-Study-Act model is promoted for quality assurance/quality improvement in healthcare. But does it have [...]
Jun
Alternative to the PDSA Model for QA/QI in Healthcare? Old-fashioned Epidemiology and Biostatistics! Part 4 of 5
Want an alternative to the Plan-Do-Study-Act (PDSA) model for quality assurance/quality improvement (QA/QI) in healthcare? [...]
2 Comments
Jul
Recommended Model for QA/QI in Healthcare: Epidemiology and Biostatistics, not PDSA! Part 5 of 5
I describe the three steps of my alternative model to the Plan-Do-Study-Act (PDSA) model for [...]
Jul
Want an alternative to the Plan-Do-Study-Act (PDSA) model for quality assurance/quality improvement (QA/QI) in healthcare? I recommend approaching QA/QI a different way, by thinking about the various functions of the QA/QI department.
Am also very much enjoying Monika’s course and the RAD concept. As a health professional entering the tech world this immersion into its terminology and yes, foreign nomenclature is immeasurable!
Thank you for your comment! I’m so glad you got a lot out of the course.